
Looking information about any correlation between cell phones and cancer? Look here:
Cell phones, Cancer and Brain Tumors
Cell phone SARs (Specific absorption rates)
QUESTION: A cellular communications tower was recently built near my home. Does this present a risk I should be worried about? Answer: These cellular towers are the base stations for the cells that make up the coverage area for a cellular telephone network. Most of these towers are 50 to 200 ft tall with an antenna mounted on top. These antennas emit radiofrequency electromagnetic waves but at a level much lower than those associated with commercial radio and television stations. The radiofrequency energy these cellular antennas radiate has a power level similar to the energy emitted by common household light bulbs. The strength of these electromagnetic fields (EMFs) decreases rapidly with distance from the antennas and the exposures usually occur hundreds of feet away. In some locations around these facilities, the strength of these fields can decrease to almost undetectable levels at the site property line. Even the peak levels seen are thousands of times lower than the limits set for human exposure to radiofrequency EMFs.
While the biological effects of exposure to much higher intensity radiofrequency fields have been somewhat determined, there is research presently underway to delineate what possible biological effects, if any, are linked to the low intensity exposures near cellular towers. Currently, there is no significant indication that chronic exposure to the EMFs around cellular sites has any potential to be hazardous to human health.
![]()
(v2.2.0, 11-Sep-99):
(v2.1.5, 5-Aug-99):
![]()
- Cross references to other questions are indicated by the letter Q followed by the question number; for example, (Q9) indicates that further information is found in Question 9.
- Technical references are shown in brackets; for example, [2] is a reference to technical note 2.
- Technical notes follow the main FAQ.
- "International notes" are appended to regular technical notes, so [International note 2] is a section within technical note 2.
![]()
1) Are there health hazards associated with living, working, playing, or going to school near a cellular phone or PCS base station antenna?
No. The consensus of the scientific community, both in the US and internationally, is that the power from these base station antennas is far too low to produce health hazards as long as people are kept away from direct access to the antennas (see Q13 and Q14 ).
![]()
Not really. There are some reasons to be concerned about human health effects from the hand-held cellular and PCS phones themselves (although it is not certain that any risks to human health actually exist). These concerns exist because the antennas of these phones can deliver large amounts of radiofrequency energy to very small areas of the user's body [83]. Base station antennas do not create such "hot spots", so the potential safety issues concerning the phones have no real applicability to the base station antennas.
For further discussion of health issues related to hand-held phones see the ICNIRP report [1], the review by Moulder et al [95], and the review by the Royal Society of Canada [99].
![]()
No. There are many technical differences between cell phones, PCS phones, and the types of "cell" phones used in other counties [2, also see international note 2]; but for evaluation of possible health hazards, the only distinction that matters is that they operate at slightly different frequencies. The radiowaves from some base stations (e.g., those for the cell phones used in the U.S.) may be absorbed by humans somewhat more than the radiowaves from other types of base stations (e.g., those for the PCS phones used in the U.S.) [23]. However, once the energy is absorbed the effects are the same.
![]()
Yes and no. The radiowaves from some antennas (particularly FM and VHF-TV broadcast antennas) are absorbed more by humans than the radiowaves from other sources (such as cellular phone or PCS base station antennas); but once the energy is absorbed the effects are basically the same.
In addition, FM and TV antennas are 100 to 5000 times more powerful than base station antennas, but are mounted on much higher towers (typically 800 to 1200 ft). ![]()
Yes. Cellular and PCS phones and their base station antennas are radios, and produce radiofrequency (RF) radiation [3]; that's how they work. This radiofrequency radiation is "non-ionizing", and its biological effects are fundamentally different from the "ionizing" radiation produced by x-ray machines [see Q6].
![]()
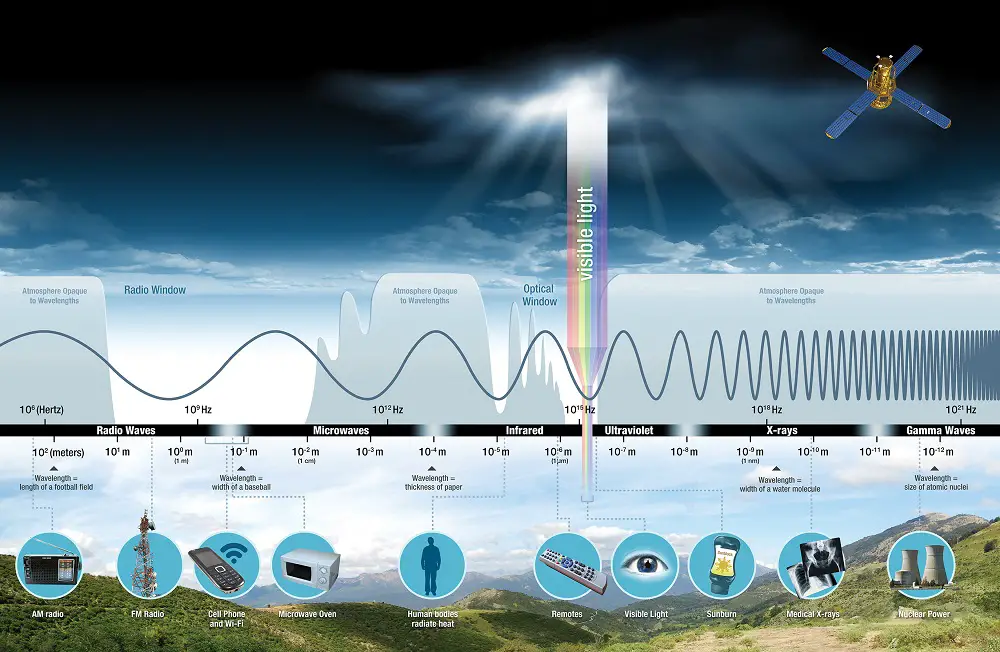
No. The interaction of biological material with an electromagnetic source depends on the frequency of the source [4]. X-rays, radiowaves and "EMF" from power lines are all part of the electromagnetic spectrum, and the parts of the spectrum are characterized by their frequency. The frequency is the rate at which the electromagnetic field changes direction and is given in Hertz (Hz), where one Hz is one cycle (change in direction) per second, and 1 megahertz (MHz) is one million cycles per second.
Electric power in the US is at 60 Hz. AM radio has a frequency of around 1 MHz, FM radio has a frequency of around 100 MHz, microwave ovens have a frequency of 2450 MHz, and X-rays have frequencies above one million MHz. Cellular phones operate at 860-900 MHz, and PCS phones operate at 1800-2200 MHz [also see international note 2].
At the extremely high frequencies characteristic of X-rays, electromagnetic particles have sufficient energy to break chemical bonds (ionization). This is how X-rays damage the genetic material of cells, potentially leading to cancer or birth defects. At lower frequencies, such as radiowaves, the energy of the particles is much too low to break chemical bonds. Thus radiowaves are "non-ionizing". Because non-ionizing radiation cannot break chemical bonds, there is no similarity between the biological effects of ionizing radiation (x-rays) and nonionizing radiation (radiowaves) [4].
The Electromagnetic Spectrum |
 |
![]()
No. Power lines produce no significant non-ionizing radiation, they produce electric and magnetic fields. In contrast to non-ionizing radiation, these fields do not radiate energy into space, and they cease to exist when power is turned off. It is not clear how, or even whether, power line fields produce biological effects; but if they do, it is not in the same way that high power radiowaves produce biological effects [4, 53]. There appears to be no similarity between the biological effects of power line "EMF" and the biological effects of radiowaves.
![]()
Yes. There are national and international safety guidelines for exposure of the public to the radiowaves produced by cellular phone and PCS base station antennas. The most widely accepted standards are those developed by the Institute of Electrical and Electronics Engineers and American National Standards Institute (ANSI/IEEE) [5], the International Commission on Non-Ionizing Radiation Protection (ICNIRP) [6], and the National Council on Radiation Protection and Measurements (NCRP) [7].
These radiofrequency standards are expressed in "plane wave power density", which is measured in mW/cm-sq (milliwatts per square centimeter) [8]. For PCS antennas, the 1992 ANSI/IEEE exposure standard for the general public is 1.2 mW/cm-sq. For cellular phones, the ANSI/IEEE exposure standard for the general public is 0.57 mW/cm-sq [9]. The ICNIRP standards are slightly lower and the NCRP standards are essentially identical [10].
In 1996 the U.S. Federal Communications Commission (FCC) released radiofrequency guidelines for the frequencies and devices they regulate, including cellular phone and PCS base station antennas [11]. The FCC standards for cellular phone and PCS base station antennas are essentially identical to the ANSI/IEEE standard [12].
The public exposure standards apply to power densities averaged over relatively short periods to time, 30 minutes in the case of the ANSI/IEEE, NCRP, and FCC standards (at PCS and cellular phone frequencies). Where there are multiple antennas, these standards apply to the total power produced by all antennas [13].
![]()
Yes. When scientists examined all the published literature on the biological effects of radiowaves they found that the literature agreed on a number of key points [see 1, 5, 6, 7, 14, 53, 83, 90, 95, 96 and 99 for details]:
ANSI/IEEE and FCC applied a 10-fold safety margin to establish occupational exposure guidelines. They then applied an additional 5-fold safety margin for continuous exposure of the general public. Finally, detailed studies were done to establish the relationship of power density, which can be routinely measured, to energy absorption, which really matters [8].
The result was a highly conservative public exposure guideline that was set at a level that is only 2% of the level where replicated biological effects have actually been observed.
![]()
No. There are differences between the standards. ANSI, ICNIRP, NCRP and FCC all use the same biomedical data, and the same general approach to setting safety guidelines. However, there are differences in the models used by the different groups, and hence there are slight differences in the final numbers [17]. No biological significance should be associated with these slight differences.
Other standards, such as the Australian standard [international note 12], are different because larger safety margins are used.
![]()
Yes. Until 1996 the FCC used an out-dated (1982) ANSI standard that was really designed for occupational, rather than public exposure. In 1996 the FCC adopted a new standard that [11] is based on the newer (1992) ANSI standard, but which is not identical to it [12].
This new FCC standard applies to all new transmitters licensed after 15-Oct-97, but existing facilities have until year 1-Sep-2000 to demonstrate compliance.
![]()
Yes. With proper design, cellular phone and PCS base station antennas can meet all safety standards by a wide margin.
A low-gain PCS and/or cellular base station antenna, mounted 40 ft off the ground and operated at the maximum possible intensity, might produce a power density as high as 0.02 mW/cm-sq on the ground near the antenna site; but ground level power densities will more often be in the 0.0001 to 0.005 mW/cm-sq range [57]. These power densities are far below all the safety standards, and the standards themselves are set far below the level where potentially hazardous effects have been seen.
Within about 500 ft of the base of the antenna site, the power density may be greater at elevations above the base of the antenna site (for example, at the second floor of a building or on a hill). Even with multiple antennas, and with both cellular phone and PCS antennas on the same tower, power densities will be less than 2% of the guidelines at all heights and at all distances of more than 170 feet from an antenna site.
Further than about 500 ft from the antenna site power density does not rise with increased elevation.
Power density inside a building will be lower by a factor of 3 to 20 than outside [54].
Peterson et al [77] measured power densities around cell phone base stations. The measurements were for 1600 W (ERP) low-gain antennas on towers that ranged from 120 to 250 feet in height. The maximum power density on the ground was 0.002 mW/cm-sq, and the maximum was at 50-200 feet from the base of the towers. Within 300 feet of the base of the towers, the average power density was less than 0.001 mW/cm-sq.
![]()
Yes. There are some circumstances under which an improperly designed cellular phone and PCS base station antenna could violate safety standards.
Safety standards for uncontrolled (public) exposure could be violated if antennas were mounted in such a way that the public could gain access to areas within 20 feet of the antennas themselves [18]. This could arise for antennas mounted on, or near, the roofs of buildings.
Safety standards for controlled (occupational) exposure could be violated if antennas were mounted on a structure where worker access to areas within 10 feet the antennas is required [18]. Peterson et al [77], for example, found that 2-3 feet from a 1600 W (ERP) low-gain roof-top antenna, the power density was as high as 2 mW/cm-sq (compared to the ANSI [9] public exposure standard of 0.57 mW/cm-sq
![]()
While specific recommendations require a detailed knowledge of the site, the antenna, and the mounting structure, some general criteria can be set.
![]()
The FCC guidelines [11] require detailed calculations and/or measurement of radiofrequency radiation for some high-power rooftop transmitters, and some high-power transmitters whose antennas are mounted on low towers [19].
In general, the above guidelines will always be met when antennas are placed on their own towers. Problems, when they exist, are generally confined to:
- Antennas placed on the roofs of buildings; particularly where multiple cellular and/or PCS base station antennas for different carriers are mounted on the same building;
- Antennas placed on structures that require access by workers (both for regular maintenance, and for uncommon events such as painting or roofing).
Because siting criteria for high- and low-gain antennas are different it is important to be able to tell them apart. Fortunately, the antennas look rather different:
Distinguish the Two Antenna Types |
 |
![]()
Even from a distance the site (towers) for high- and low-gain antennas look different. When high-gain antennas are mounted on buildings, they may not be obvious, particularly if they are mounted to the sides of building, or more commonly to the sides of penthouses.
Diffent Ways to Mount Antennas |
 |
![]()
The RF patterns for the two different types of antennas are very different. For a low-gain (whip) antenna of the type used by most cell phone bases stations, the pattern looks like this:
RF Emissions from a 1000 W ERP Low-Gain Antenna |
 |
![]()
Very close to a low-gain antenna (in what is technically known as the "near field"), the power density around an antenna looks like this:
RF Emissions from a 1000 W ERP Low-Gain Antenna |
 |
The data for the above figure were adapted (with permission) from drawings provided by UniSite Inc. of Tampa, Florida (http://www.unisite.com).
![]()
For a high-gain (sector) antenna of the type used in PCS base stations, the pattern looks like this:
RF Emissions from a Single 1000 W ERP High-Gain Antenna |
 |
![]()
Keep in mind that a typical PCS base station will use 3 (or occasionally 4) of these transmission antennas, all pointing in different directions.
Very close to a single high-gain antenna (in what is technically known as the "near field"), the power density around an antenna looks like this:
RF Emissions from a Single 1000 W ERP High-Gain Antenna |
 |
The data for the above figure were adapted (with permission) from drawings provided by UniSite Inc. of Tampa, Florida (http://www.unisite.com).
![]()
In general this will not be a problem.
No. Radiofrequency safety guidelines do not require either setbacks or use restrictions around cellular or PCS base station antenna sites, since power levels on the ground are never high enough to exceed the guidelines for continuous public exposure (see Q8 and Q12).
As discussed in Q13 and Q14, there may be circumstances where use restrictions will have to be placed around the antennas themselves.
![]()
Not everyone. Even among scientists there are a few people who claim that there is evidence that low level exposure to RF is hazardous (see, for example, Q15B and Q15C). However, not even these scientists would argue that power densities as low as those found around properly-designed base station antenna sites are hazardous.
![]()
Yes. The EPA asked the FCC to adopt parts of the 1986 NCRP guidelines [7] rather than the entire 1992 ANSI guidelines [5]. This the FCC did [11], and EPA has formally endorsed the FCC safety standards.
In a 25-Jul-96 letter to Reed Hunt (Chairman of the FCC), Carol Browner (Director of EPA) wrote:
"We have reviewed... 'FCC Draft of July 2, 1996, in the Matter of Guidelines for Evaluating The Environmental Effects of Radiofrequency Radiation'. This new approach... addresses our concerns about adequate protection of public health. I commend you for taking this approach..."
In a 17-Jan-97 follow-up letter to Reed Hunt (Chairman of the FCC), Mary Nichols (EPA Assistant Administrator for Air and Radiation) wrote:
"I would like to reiterate EPA's support of FCC's final RF exposure guidelines issued in August [of 1996] as providing adequate protection of public health."
In a 30-April-1999 letter to the FCC, Robert Brenner (EPA Acting Deputy Assistant Administrator for Air and Radiation) stated:
"The FCC guidelines expressly take into account thermal effects of RF energy, but do not directly address postulated non-thermal effects, such as those due to chronic exposure. That is the case largely because of the paucity of scientific research on chronic, non-thermal health effects. The information base on non-thermal health effects has not changed significantly since the EPA's original comments in 1993 and 1996. A few studies report that at non-thermal levels, long term exposure to RF energy may have biological consequences. The majority of currently available studies suggests, however, that there are no significant non-thermal human health hazards. It therefore continues to be EPA's view that the FCC exposure guidelines adequately protect the public from all scientifically established harms that may result from RF energy fields generated by FCC licensees."
![]()
Yes and no. That claim was made in 1996, but follow-up studies in Australia (see below) and in the UK (see Q15D) contradict this claim.
Hocking and colleagues [28] published an "ecological" epidemiology study that compares municipalities "near TV towers" to those further away. No RF exposures were actually measured, but the authors calculate that exposures in the municipalities "near TV towers" were 0.0002 to 0.008 mW/cm-sq. No other sources of exposure to RF are taken into account, and the study is based on only a single metropolitan area. The authors report an elevated incidence of total leukemia and childhood leukemia, but no increase in total brain tumor incidence or childhood brain tumor incidence.
More detailed epidemiology studies of FM/TV antennas in the U.K. have not found evidence for a cancer connection (see Q15D).
In 1998, McKenzie and colleagues [62] repeated the Hocking study [28]. McKenzie and colleagues looked at the same area, and at the same time period; but they made more precise estimates of the RF exposure that people got in various areas. They found increased childhood leukemia in one area near the TV antennas, but not in other similar areas near the same TV antennas; and they found no significant correlation between RF exposure and the rate of childhood leukemia. They also found that much of the "excess childhood leukemia" reported by Hocking et al occurred before high-power 24-hour TV broadcasting had started. This replication study, plus the failure to find any effect in the larger UK studies (see Q15D), suggests that correlation reported by Hocking et al [28] was an artifact.
![]()
Yes. In a 1995 article labeled an "opinion piece", Goldsmith [29A] argues that there is evidence that RF exposure is associated with mutations, birth defect, and cancer. This review is based largely on what the author admits to be "non-peer-reviewed sources", most of which are stated to be "incomplete" and to lack "reliable dose estimates". The author further states that "no systematic effort to include negative reports is made; thus this review has a positive reporting bias".
In an article based on a 1996 meeting presentation [29B] Goldsmith argues that epidemiological studies "suggest that RF exposures are potentially carcinogenic and have other health effects". His conclusions are based largely on:
- studies of RF exposure at the US embassy in Moscow (see Q16 and Hill [68]);
- the "geographical correlation" studies of Hocking et al [28] and Dolk et al [34, 35] that are discussed in Q15B and Q15D;
- the study of Korean war radar operators by Robinette et al [67] that is discussed in Q16.
Few scientists agree with the opinions expressed by Goldsmith (see, for examples the reviews of the RF epidemiology in 1, 5, 6, 7, 14, 53); and even fewer would be willing to base a conclusion on the types of data sources that Goldsmith relies on.
![]()
Yes and no. Dolk and colleagues [34] investigated a reported leukemia and lymphoma cluster near a high-power FM/TV broadcast antenna at Sutton Coldfield in the UK. They found that the incidence of adult leukemia and skin cancer was elevated within 2 km of the antenna, and that the incidence of these cancers decreased with distance. No associations at all were seen for brain cancer, male or female breast cancer, lymphoma or any other type of cancer.
Because of this finding, Dolk and colleagues [35] extended their study to 20 other high-power FM/TV broadcast antennas in the UK. Cancers examined were adult leukemia, skin melanoma and bladder cancer, and childhood leukemia and brain cancer. No elevations of cancer incidence were found near the antennas, and no declines in cancer incidence with distance were seen. This large study does not support the results found in the much smaller studies by the same authors at Sutton Coldfield [34] or by Hocking et al [28] in Australia.
![]()
Yes and no. Roger Coghill (U.K.) and Neil Cherry (New Zealand) have been quoted in the mass media as claiming that there is evidence that RF exposure is hazardous at intensities well below the ANSI, FCC, ICNIRP and NRPB guidelines.
Roger Coghill appears to be an "environmental manager", who runs a laboratory that makes [permanent?] magnets "to help people suffering from muscular or arthritic pain" [59]. He has self-published a document [58] that explains "Coghill's hypothesis of cerebral morphogenic radiation". Apparently, Coghill believes that "the brain is actually a organic fully operational radio transmission station... that is in radio contact with every cell in its body" [59]. He appears to base his theory heavily on "Eastern European" research that has not been published in the West [59].
Neil Cherry is an elected official from New Zealand. and a "Senior Lecturer in Agricultural Meteorology" [60]. Like Coghill, he has self-published a document on the hazards of exposure to low-intensity RF [60]. Cherry has been quoted in the mass media as saying that "EMF exposure" is "highly statistically associated with health effects although there is no scientific proof that EMF caused the health effects" [61]. According to Cherry, these health effects include "cancer at many sites in the body, sleep disruption, chronic fatigue syndrome, miscarriage, birth defects, altered human EEG and circadian rhythms and several other adverse effects." [61]. Cherry's ideas appear to depend heavily on the views of Goldsmith (Q15C) and Hocking (Q15B).
Neither Coghill nor Cherry have published anything in the peer-reviewed scientific literature to support their claims. Both Coghill and Cherry mix discussions of power-frequency fields and RF as though they were biologically equivalent (which is almost certainly not correct), and to rely heavily on unpublished and non-reviewed sources (which are impossible to check). Their comments to the mass media have been very vague as to the scientific basis for their opinions. Until Coghill and Cherry present their theories in a peer-reviewed scientific forum, and back their theories with actual data, it is impossible for any scientist to take their theories seriously.
![]()
Yes and no. Dr. Henry Lai (Department of Bioengineering, University of Washington, Seattle) has claimed at meetings that "low intensity" RF radiation has effects on the nervous system of rats. Dr. Lai has further claimed at meetings that there are published studies showing that RF radiation can produce "health effects" at "very low field" intensities.
Dr. Lai's own research has no obvious relevance to the safety of cell phone base stations since most of his studies were conducted with RF radiation intensities far above those that would be encountered near base stations. In general, Dr. Lai's studies were done with at a power density of 1 mW/cm-sq and an SAR of 0.6 W/kg [31, 92, 93]. This RF radiation intensity is over 100 times greater than that would be encountered in publicly-accessible areas near FCC-compliant base stations [16], and substantially exceeds the SAR limit that forms the basis of the FCC [11] and ANSI [5] safety guidelines for public exposure [17]. For further discussion of the research on possible effects of RF radiation on the nervous system see reviews by Lai [93] and Juutilainen and de Seze [90].
At a meeting in Vienna in 1998, and in a letter sent to public officials in 1999, Dr. Lai referenced six studies in support of his claim that there is data showing that RF radiation can produce "health effects" at "very low field" intensities. These studies were:
![]()
Yes and no. While there have been no epidemiology studies of cancer and cell phone base stations, there have been epidemiology studies of cancer and other types of exposure to radiowaves. For a recent review see Elwood [94].
In general, epidemiology studies of radiowaves and cancer have not found significant correlations between exposure and cancer. The studies include:
- studies of cancer in people occupationally exposed to radiowaves,
- geographic correlation studies that compare cancer rates among areas with different potential exposures to radiowaves,
- "cancer cluster" studies.
Geographic correlation studies (see Q15B, Q15D and Elwood [94]) estimate the strength of radiowaves in geographic areas and correlate these estimates with disease rates in these areas. Even when the design of geographic correlation studies is optimal, they are considered exploratory and are not used for determining causality.
Reports of clusters of cancer provide little practical information. The major steps in evaluating reports of "cancer clusters" are:
- define a logical (as opposed to arbitrary) boundary in space and time,
- determine whether an excess of a specific type of cancer has actually occurred,
- identify common exposures and characteristics.
The above steps, however, have not generally been followed in studies of radiowaves, and reports of "cancer clusters" are of essentially no value in determining whether exposure to radiowaves is a cause of cancer (see Elwood [94] for details of these studies).
The majority of the occupational studies of radiowaves exposure have deficiencies in exposure assessments because occupation or job title was used as an estimate of exposure; that is, actual radiowave exposure levels are not known.
There are three epidemiological studies that are generally considered to have acceptable design and analysis, adequate sample size, and sufficient follow-up time: Robinette et al [67], Hill [68] and Milham [69]. These three studies do not show statistically-significant associations between radiowave exposure and either cancer in general or any specific kind of cancer.
The other studies of acceptable design (Lilienfeld et al [70], Lagorio et al [71], Muhm [72], Tynes et al [73], Grayson et al [33]) have more limitations in exposure assessment, case ascertainment, or follow-up time; but they also do not suggest that radiowave exposure increases the risk of either cancer in general or any specific kind of cancer.
Szmigielski [79] studied Polish military personnel who may have had radiowave exposure. The incidence of cancer of all types, brain cancer, leukemia and lymphoma are reported to be elevated in exposed personnel. Because the methods of data collection and analysis are inadequately described or unsuitable, and because assessment of radiowave exposure is very deficient, the report does not meet basic epidemiological criteria for acceptability. Elwood [94] also concludes that the methods used in the Szmigielski study may have created a systematic bias "that would be expected to produce an increased relative risk for all types of cancer".
In a study that received extensive press coverage even before it was published, Hardell et al [79] assessed mobile phone use in several hundred Swedish brain tumor patients. They found no increased risk of brain tumors in the mobile phone users, with an odds ratio of 0.8-1.2 (that is, no effect). No increase in brain tumor incidence was seen for either analog (NMT) or digital (GSM) phone users and there was no trend towards increased risk with increased years of use or increased hours of use per year. When the data was analyzed to look only at brain tumors on the side of the head where the phone was used, there was no increase in brain tumor incidence. The authors do report that mobile phone users were more likely to get certain types of brain tumors on the side of the head where the phone was used, but the trend was not statistically significant, and was found only in the analog phone users (only this last finding was mentioned in most of the press reports).
The lack of associations between exposure to radiowaves and total cancer, and the lack of consistent associations between exposure to radiowaves and any specific type of cancer, suggests that radiowaves are unlikely to have a strong causal influence on cancer.
In his recent review of the RF epidemiology literature, Elwood [94] concluded that:
Several positive associations suggesting an increased risk of some types of cancer in those who may have had greater exposure to RF emissions have been reported. However, the results are inconsistent: there is no type of cancer that has been consistently associated with RF exposures. The epidemiologic evidence falls short of the strength and consistency of evidence that is required to come to a reasonable conclusion that RF emissions are a likely cause of one or more types of human cancer. The evidence is weak in regard to its inconsistency, the design of the studies, the lack of detail on actual exposures, and the limitations of the studies in their ability to deal with other likely relevant factors. In some studies there may be biases in the data uses.
![]()
Possibly, but there is no replicated evidence for such effects. It has been suggested that amplitude-modulated (AM) RF radiation might have different effects than continuous-wave (CW, unmodulated) RF radiation. This could be important, since cell and PCS phones and base stations produce a modulated signal, and much of the research has been done with unmodulated RF sources.
This issue had been reviewed in detail by Juutilainen and de Seze [90] who concluded that:
"The literature relevant to the possible biological effects of AM radiofrequency radiation consists of scattered observations using a wide variety of experimental models and exposure parameters... Several studies have reported findings consistent with effects on the nervous system and cancer-related biological processes. However, the methods and exposure parameters vary widely, and no independent replications of the positive finds have been reported. The results available today fail to support the existence of well-defined modulation-specific bioeffects from exposure to radiofrequency radiation."
![]()
Possibly. Some groups in the general population might be more sensitive to the effects of radiowaves than others, but no such groups have actually been found. The possible existence of such sensitive individuals is one of the main reasons that an additional 5-fold safety margin is added to the public exposure guidelines (see Q9).
![]()
Although the public's principle health concern about cell phone and PCS base station antennas appears to be the possibility of a cancer connection (see Q21 and Q23C-Q23E), other health-related issues come up periodically. Particularly common are questions about interference with heart pacemakers (covered in Q19A). This section will also cover less common issues. The possibility of a connection with miscarriages and birth defects is covered in Q22.
![]()
No. There is no evidence that cellular phone or PCS base station antennas will interfere with cardiac pacemakers or other implanted medical devices as long as exposure levels are kept within the ANSI standard for uncontrolled exposure (see Q8 and Q12).
It is possible that PCS phones themselves might interfere with pacemakers if the antenna is placed directly over the pacemaker. This problem is reported to occur with only some types of PCS phones and some types of pacemakers [46].
![]()
There is no reason to think so. There are anecdotal reports that cell phones cause headaches (see Frey [48], and the discussion of Mild et al and Sandstrom et al [25] in Q23). There have been no serious epidemiological studies of the issue, and there are no real biophysical or physiological bases for expecting a connection.
![]()
There are unreplicated reports of such things. Braune et al [82] reported that human volunteers using a 2 W GSM cell phone for 35 minutes showed a 5-10 mm Hg rise in blood pressure. The study is small and was not blinded, and a rise in blood pressure of this magnitude has no known health consequences. Eulitz et al [84] reported that cell phones can alter the electrical activity of the brain. However, the effect may be an artifact caused by RF interference with the EEG leads.
In 1999, Preece et al [97] reported that exposure of human volunteers to cell phone RF radiation might decrease reaction times. The press coverage was extensive, but the actual study is not particularly impressive:
For an up-to-date review of the behavioral effects of RF radiation see D'Andrea [96].
![]()
Yes. If exposure is sufficiently intense, radiowaves can cause biological effects. Possible injuries include cataracts, skin burns, deep burns, heat exhaustion and heat stroke. Most, if not all, of the known biological effects from exposure to high-power radiofrequency sources are due to heating [20]. The effects of this heating range from behavioral changes to eye damage (cataracts) [see refs in 1, 5, 6, 7 14, 53, 83 and 90]. Except possibly within a few feet of the antennas themselves [18], the power produced by cellular phone and PCS base station antennas is too low to cause heating.
There have been scattered reports of effects [21] that do not appear to be due to heating, the so called non-thermal effects [20]. None of these effects have been independently replicated, and none have any obvious connections to human health risks.
![]()
No. Even at high levels of exposure, there is no substantial evidence that radiowaves can either cause or contribute to cancer (for an opinion to the contrary see the reports discussed in Q15B and Q15C). Although research in this area has been extensive, there is no replicated laboratory or epidemiological evidence that radiowaves at the power levels associated with public exposure to radiowaves from cellular phone and PCS base station antennas are associated with cancer [see refs in 1, 5, 6, 7, 14, 74 and 83 for details].
There are two recent laboratory reports that RF exposure might produce cancer, or cancer-related injuries in animals. These studies are discussed in Q23C and Q23E. Both studies use RF levels far above those found in publicly-accessible area near base station antennas, and neither study has been replicated.
The epidemiological studies of RF show no consistent association with total cancer, or with any specific type of cancer (see Q16).
![]()
Indirectly, yes. Exposure to levels of radiowaves sufficient to cause whole body heating can cause miscarriages or birth defects. The power produced by cellular phone and PCS base station antennas is far too low to cause such heating. There is no laboratory or epidemiological evidence at all that radiowaves at the power levels associated with public exposure to radiowaves from cellular phone and PCS base station antennas are associated with miscarriages or birth defects [see refs in 1, 5, 6, 7 and 14 for details].
See also the discussion of Bastide et al [26] in Q23A.
![]()
There is a constant flow of new information. This section will attempt to summarize this new information. Studies which attract major attention will often get their own sections, such as the epidemiological studies discussed in Q15B, Q15C, Q15D and Q15E, the mouse studies discussed in Q23C and Q23D, and the DNA strand break studies discussed in Q23E.
![]()
At the 1998 meeting of the Bioelectromagnetics Society (BEMS), the principle meeting where biological and health effects of radiowaves are discussed), there were numerous papers that dealt with radiowaves and/or personal communication systems. Similarly, at the 2nd World Congress of Electricity and Magnetism in Medicine and Biology in June 1997, there were many papers that dealt with radiowaves and/or personal communication systems. None of these papers reported replicated results that would suggest that exposure to radiowaves at levels allowed by the 1992 ANSI standard [5] would pose any health risk to humans.
A number of the reports dealt with dosimetry issues for the hand-held phones themselves. Among these:
- Santani et al [22]: RF exposure from European GSM digital phones (and by analogy US digital PCS phones) was greatest during establishment of the call and when the user was in an area with poor reception quality.
A number of reports dealt with electromagnetic interference issues, but none of these reports add much to the information presented in the publication by Hayes et al [46].
Among the biological studies reported at the 1998 BEMS meeting, those with the possible relevance to the issue of human health effects of radiowaves were:
- Mild et al and Sandstrom et al [25]: An epidemiological study of mobile phone users in Sweden reported that users of the older analog system (similar to the US cellular system) reported more headaches than the users of the newer digital GSM system (similar to the US PCS system). There was no control group of non-users as the investigators found that it was "absolutely impossible to find controls" who had similar life-styles but did not use mobile phones.
- Bastide et al [26]: Increased mortality was seen in chick embryos exposed continuously for 21 day to RF from commercial cell phones. Exposure was for 24-hrs per day, using 2 W phones (compared to the 0.4-0.6 W used by most U.S. cell and PCS phones) placed 1 cm from the eggs. Neither power-density or SAR were reported, and heating effects cannot be ruled out.
![]()
Relevant peer-reviewed publications from 1997-1999 include:
- Dolk et al [34 and 35]: A geographical correlation study of cancer that is discussed in Q15D.
- Repacholi et al [37]: A mouse lymphoma study that is discussed in Q23C.
- Vijayalaxmi et al [41]: A cellular genotoxicity study that is discussed in Q23E.
- Cain et al [42]: A cellular genotoxicity study that is discussed in Q23E.
- Toler et al [45]: An animal carcinogenicity study that is discussed in Q23D.
- Malyapa et al [49]: Three papers reporting attempts to confirm the Lai and Singh [31] studies that are discussed in Q23E.
- Frei et al [44]: An animal carcinogenicity study that is discussed in Q23D.
- McKenzie et al [49]: An attempt to replicate the geographical correlation study of Hocking et al [28] that is discussed in Q15B.
- Lagorio et al [71]: An occupational epidemiology study that is discussed Q16.
- Imaida et al [63]: A liver tumor promotion study that is discussed in Q23D.
- Braune et al [82]: Human volunteers using cell phones showed a rise in blood pressure. See Q19C.
- Kwee and Rasmark [76]: RF exposure at 960 MHz (SAR = 0.00002-0.002 W/kg) caused a slight decrease in the growth rate of cultured human cells (see further discussion in Q15F).
- Antonopolous et al [75]: A study of cell growth and genotoxicity that is discussed Q23E.
- Phillips et al [78]: A study of cellular genotoxicity that is discussed Q23E and Q15F.
- Verschaeve and Maes [80]: A review of RF genotoxicity studies that is discussed in Q23E.
- Brusick et al [81]: A review of RF genotoxicity studies that is discussed in Q23E.
- Eulitz et al [81]: Human volunteers using cell phones showed changes in brain activity. See Q19C.
- Goswami et al [87] reported that 835-848 MHz RF radiation at a SAR of 0.6 W/kg did not trigger a general stress response in cultured mammalian cells.
- Chagnaud and Veyret [91] reported that exposure of rats to a 900 MHz cell phone signal at 0.05 and 0.2 mW/cm-sq (SAR of 0.075 and 0.27 W/kg) had no effect on their immune system.
- Moulder et al [95]: A review of the evidence for a causal association between cell phone RF radiation and cancer.
- D'Andrea [96]: A review of the behavioral effects of RF radiation.
- Preece et al [97]: Effects of RF on brain function discussed in Q19C.
- Hardell et al [100]: No excess incidence of brain tumors in mobile phone users, discussed in Q16C.
- Adey et al [24]: No excess incidence of brain tumors in rats exposed for life-time to pulse-modulated RF. See Q23D.
![]()
A 1997 study [37] reports that lymphoma-prone mice exposed for 18 months to strong, but intermittent, radio-frequency fields of the type used by digital cellular phones have an increased incidence of lymphomas. No increases in the incidence of other types of tumors were found. The field intensities used are above the guidelines for public exposure recommended in the ANSI/IEEE standard (Q8), and are far above those that exist in publicly-accessible areas near cellular phone and PCS base station antennas [16].
While this study is very interesting, its impact on regulation of RF exposure of the general public is quite unclear:
See the Technical notes for the reference [37], quotes from the authors' abstract [38], quotes from the authors' discussion [39], and for further technical details [40].
Several questions have been repeatedly asked about this study:
No. Before this study can be related to human risk assessment:
- it must be replicated,
- a similar study must be done with normal mice,
- the exposure-response relationship for the effect must be known,
- the induction of other types of tumors must be studied.
When you want to know whether something might cause cancer, you usually start with a sensitive strain of animals and a high dose of the agent. This maximizes your chance of finding something. If you find nothing under these circumstances, then you can be fairly confident that the agent does not cause this cancer. If you do find excess cancer, you then need to determine whether this will also happen in normal animals and/or at more reasonable doses. If you first do normal animals at low doses, and you find no excess cancer, you still would need to test cancer-prone animals at high doses.
An additional problem with using normal mice and low doses of RF to study induction of lymphoma, is that lymphoma is rare in normal mice (1-3% lifetime incidence). To detect a 50% increase in this normal rate would require over 2000 mice.
There are at least 10 other studies of long-term exposure of rodents to radiofrequency radiation. None of these studies used lymphoma-prone mice and none have reported excess lymphoma. See Q23D for details.
It is not easy to expose animals to uniform levels of RF. If animals are unrestrained in cages, the RF dose (the SAR [8]) varies with the position of the animal, with its orientation to the antenna, with the presence of other animals, and with the animal size. To get well-defined RF doses, the animals must be confined in small holders, and the daily handling and confinement this requires can produce biological effects all by itself. Even under these conditions, the SAR may change as the animals increase in size. Basically, the experimenter has a choice: treat free-running animals with minimal disturbance and accept uncertain dosimetry, or get good dosimetry and risk artifacts due to handling and confinement. Either choice is open to criticism.
There are at least 10 other studies of long-term exposure to rodents to RF.
- In 1971, Spalding el al [64] published a study of mice that had been exposed to 800-MHz RF for 2 hr/day, 5 days/week, for 35 weeks at a SAR of 13 W/kg. The average life span of the RF-exposed group (664 days) was slightly, but not significantly, longer than that of the sham group (645 days).
- In 1982 Szmigielski et al [65] published a study of mice that were exposed to 2450-MHz RF for 2 hr/day, 6 days/wk, for up to 6 months. Exposures were at 2-3 and 6-8 W/kg. Controls included both sham-irradiated animals and animals subject to "confinement stress". Both RF exposure and confinement stress significantly accelerated the appearance of both chemically-induced skin tumors and chemically-induced breast tumors. The dosimetry in this study is questionable, and seems likely that the mice exposed at the higher dose were subjected to physiologically-significant heating.
>In 1988 Saunders et al [98] published a study of male mice that were exposed to 2450-MHz RF radiation (power density of 10 mW /cm-sq and SAR of 4 W/kg) for 6 h per day for a total of 120 h over an 8-week period. At the end of the treatment the mice were mated with unexposed females. There was no significant reduction in pregnancy rate, so that there had been no increase in dominant lethal mutations. Examination of spermatogonia showed no increase in chromosome aberrations. The authors conclude that "there is no evidence in this experiment to show that chronic exposure of male mice to 2450-MHz microwave radiation induces a mutagenic response".
- In 1994 Liddle et al [66] published a study that examined the effects of life-time 2450-MHz RF exposure in mice. Mice were exposed for 1 hr/day, 5 days/week throughout their life at either 2 or 6.8 W/kg. Life span was significantly shortened in mice exposed at 6.8 W/kg (median of 572 days vs 706 days in the sham-exposed group). However, at 2 W/kg, the RF-exposed animals lived slightly, but not significantly longer (median of 738 days) than the sham-exposed group. The authors suggested that the heating from exposure at 6.8 W/kg was stressful enough to decrease life span.
- In 1992, Chou et al [43] published a study of 100 normal rats that were exposed to pulsed 2450 MHz RF at 0.15-0.40 W/kg [8] for 21.5 hrs/day and 25 months. No effects were observed on life-span or cause of death. An increase in total cancer was seen in exposed group, with no effect on survival. The malignancy rates in the controls was unusually low for this strain, and no increase in benign tumors were observed.
Two primary lymphomas were seen in the exposed animals, and two in the controls. No benign or malignant brain tumors were seen in either exposed or control rats.
The authors concluded: "Microwave exposure... showed no biologically significant effects on general health... The findings of an excess of primary malignancies in exposed animals is provocative. However, when this single finding is considered in light of other parameters, it is conjectural whether the statistical difference reflects a true biological influence. The overall results indicate that there are no definitive, biologically significant effects...".
- In 1994, Wu et al [56] published a report on 26 mice that were exposed to a chemical carcinogen plus 2450 MHz RF at 10 mW/cm-sq (10-12 W/kg). Exposure continued for 3 hrs/day, 6 days/week for 5 months. The chemical carcinogen is one that causes colon cancer. No difference in colon cancer rates were seen between animals treated with the carcinogen alone and the animals treated with the carcinogen plus RF.
- In 1997, Toler el [45] published a report on 200 mammary-tumor-prone mice exposed to pulsed 435 MHz RF at 1.0 mW/cm-sq (0.32 W/kg). Exposure continued for 22 hrs/day, 7 days/week for 21 months. The authors reported no differences in survival or mammary tumor incidence. The authors reported that there was no difference in the rates of any types of tumors between the exposed and the control group. Of particular note, there was no difference in the lymphoma, leukemia or brain tumor rate between the exposed and the control group.
- In 1998, Frie et al [44] published a report on 100 mammary-tumor prone mice that were exposed to 2450 MHz RF at a SAR of 0.3 W/kg. Exposure was for 20 hrs/day, 7 days/week for 18 months. The study found no difference in tumor incidence or survival between the exposed and the control group. Later in 1998, Frie et al [47] published a second study using the same mouse model and the same exposure regimen, but a higher SAR of 1.0 W/kg. Again, the study found no difference in tumor incidence or survival between the exposed and the control group. There were no differences in lymphoma, leukemia or brain tumor incidence between the exposed and the control group in either study.
- In 1998 Imaida et al [63a] published a report on 48 rats that were given a chemical carcinogen that cause liver cancer, and were then exposed to 929 MHz RF an a SAR of 0.6-0.9 W/kg. Exposure was for 90 min/day, 5 days/week for 6 weeks. No difference in liver cancer rates were seen between RF-exposed rats and rats given only the chemical carcinogen.
In a second 1998 paper, Imaida et al [63b] reported a similar lack of liver cancer promotion in rats exposed to 1500 MHz RF at a SAR of 2.0 W/kg. Again, exposure was for 90 min/day, 5 days/week for 6 weeks.
![]() At the 1996 BEMS meeting, Adey et al reported that exposure to pulse-modulated 837 MHz RF did not increase brain tumor incidence in rats; and at the 1997 World Congress, Adey et al [50] reported a similar lack of effect for frequency-modulated RF. The pulsed-field study was finally published in 1999 [24], but the study with frequency-modulated RF has still not been published. In the published study, RF exposure started with continuous whole-body far-field exposure of pregnant rats and continued through weaning. At 7 weeks of age, localized near-field exposure of the head was begun, and this exposure continued for 22 months (2 hrs/day, 7.5 min on - 7.5 min off, 4 days/week). Some rats were also treated with a chemical brain tumor carcinogen (ethylnitrosourea, ENU). Brain SARs ranged from 0.7 to 1.6 W/kg, and whole-body SAR ranged from 0.2 to 0.7 W/kg; the range of SARs was due to changes in weight and variability in animal positioning. The number of brain tumors was less in the RF-exposed groups than in the sham-exposed groups, but the difference was not statistically significant. This non-significant decrease was seen in both rats treated with RF alone, and in rats treated with RF plus the chemical brain tumor carcinogen. According to the meeting report [50], the design of the study using frequency-modulated RF was similar, and no effect on brain tumor incidence was seen.
At the 1996 BEMS meeting, Adey et al reported that exposure to pulse-modulated 837 MHz RF did not increase brain tumor incidence in rats; and at the 1997 World Congress, Adey et al [50] reported a similar lack of effect for frequency-modulated RF. The pulsed-field study was finally published in 1999 [24], but the study with frequency-modulated RF has still not been published. In the published study, RF exposure started with continuous whole-body far-field exposure of pregnant rats and continued through weaning. At 7 weeks of age, localized near-field exposure of the head was begun, and this exposure continued for 22 months (2 hrs/day, 7.5 min on - 7.5 min off, 4 days/week). Some rats were also treated with a chemical brain tumor carcinogen (ethylnitrosourea, ENU). Brain SARs ranged from 0.7 to 1.6 W/kg, and whole-body SAR ranged from 0.2 to 0.7 W/kg; the range of SARs was due to changes in weight and variability in animal positioning. The number of brain tumors was less in the RF-exposed groups than in the sham-exposed groups, but the difference was not statistically significant. This non-significant decrease was seen in both rats treated with RF alone, and in rats treated with RF plus the chemical brain tumor carcinogen. According to the meeting report [50], the design of the study using frequency-modulated RF was similar, and no effect on brain tumor incidence was seen.
Thus it would appear that induction of lymphoma, and tumors in general, by life-time exposure of rodents to RF is not a general phenomena.
![]()
Agents that can damage the DNA of cells are presumed to have carcinogenic potential [4]. Agents that can damage DNA are called genotoxins, or are referred to as having genotoxic activity. In general, studies of cells exposed to RF have not found evidence for genotoxicity unless the SAR was high enough to cause thermal (heat) injury [5, 6, 7, 14].
In 1995 and 1996, Lai and Singh [31] reported that RF caused DNA damage (genotoxic injury) in rats. In these experiments, rats were exposed to 2450 MHz RF at 0.6 and 1.2 W/kg. After exposure, the animals were killed, and their brain cells were analyzed for DNA injury. The authors reported an increase in DNA stand breaks 4 hours after exposure.
The work of Lai and Singh [31] has failed independent attempts at replication. In 1997, Malyapa et al [49a, 49b] reported that they could not detect the effect seen by Lai and Singh, but there were some differences between the studies. In 1998, Malyapa et al [49c] reported that they could not detect the effect in an exact replicate of the Lai and Singh [31] study.
Three other recently published studies on the genotoxic potential of RF have reported no evidence for genotoxicity (damage to DNA):
- Vijayalaxmi et al [41a, 41b] found no evidence for genotoxic injury in the blood cells of mice exposed to 2450 MHz RF for 18 months at 1 W/kg, or in human lymphocytes exposed in cell culture to 2450 MHz RF at 12.5 W/kg.
- Cain et al [42] found no effect of 836 MHz RF exposure at 0.015 W/kg on neoplastic cell transformation in animal fibroblasts.
- Antonopoulos et al [75] found no effects of RF exposure on cell growth or chromosome injury in human lymphocytes. Cells were exposed to RF for 48-72 hrs at 380 MHz (SAR=0.08 W/kg), 900 MHz (SAR=0.2 W/kg) or 1800 MHz (GSM, SAR=1.7 W/kg).
Four other recently published studies found some evidence for RF exposure might be genotoxic:
- Maes et al [32] reported that exposure of human blood cells to 954 MHz RF at 1.5 W/kg did not cause chromosome damage, but increased the amount of chromosome damage produced by a chemical carcinogen.
- Scarfi et al [36] reported that exposure of animal white blood cells to 9000 MHz RF at 70 W/kg produced caused genotoxic injury and enhanced the genotoxic injury caused by a chemical carcinogen. However, the SAR in this experiment was high enough to cause thermal (heat) injury, so the relevance to real-world human exposure is unclear.
- Phillips et al [78] exposed mammalian cells to RF for 2 or 21 hours at 814 or 827 MHz. The SAR was 0.0002 or 0.002 W/kg. Both increases and decreases in the incidence of DNA strand breaks were observed, with no obvious pattern.
Two reviews of the genotoxic potential of RF were published in 1998.
Verschaeve and Maes [80] concluded that:
"According to a great majority of papers, RF fields, and mobile telephone frequencies in particular, are not genotoxic: they do not induce genetic effects in vitro [in cell culture] and in vivo [in animals], at least under non-thermal conditions [conditions that do not cause heating], and do not seem to be teratogenic [cause birth defects] or to induce cancer."Brusick et al [81] concluded that:
"The data from over 100 studies suggest that RF radiation is not directly mutagenic and that adverse effects from exposure of organisms to high power intensities of RF radiation are predominantly the result of hyperthermia [heating]; however, there may be some subtle indirect effects on the replication and/or transcription of genes under relatively restricted exposure conditions."
![]()
The documentation of the various radiofrequency standards [5, 6, 7 and 14] contain extensive references. Reasonably up-to-date reviews of this area include: the ICNIRP publication on hand-held phones [1], the review by Stuchly [83], and the review by Repacholi [74].
![]()
This FAQ sheet was written by Dr. John Moulder, Professor of Radiation Oncology, Radiology and Pharmacology/Toxicology at the Medical College of Wisconsin. Dr. Moulder has taught, lectured and written on the biological effects of non-ionizing radiation and electromagnetic fields for over two decades.
The original version of this FAQ was written in 1995 under a contract with the City of Brookfield, Wisconsin.
Parts of this FAQ are derived from three peer-reviewed publications:
- JE Moulder and KR Foster: Biological effects of power-frequency fields as - KR Foster, LS Erdreich, JE Moulder: Weak electromagnetic fields and cancer in the context of risk assessment. Proc IEEE, 85:733-746, 1997.
- JE Moulder: Power-frequency fields and cancer. Crit Rev Biomed Eng 26:1-116, 1998.
- JE Moulder, LS Erdreich, RS Malyapa, J Merritt, WF Pickard, Vijayalaxmi: Cell phones and cancer: What is the evidence for a connection? Radiat. Res., In press, 1999.
Dr. Moulder maintains similar "FAQ" documents on "Powerlines and Cancer" and "Static EM Fields and Cancer".
![]()
1. International Commission on Non-Ionizing Radiation Protection: Health issues related to the use of hand-held radiotelephones and base transmitters. Health Physics 70:587-593, 1996.
2. PCS (Personal Communication Systems) phones are hand-held radiotelephones that use a digital, rather than the analog transmission system used by most cellular phones. In the U.S., cellular phones operate at 860-900 MHz, while PCS phones operate at 1800-2200 MHz. In appearance, cellular and PCS phones and their base station antennas are similar. In the U.S., "cordless" phones operate at 46-60 MHz and "citizens band (CB)" transceivers operate at about 27 MHz.
International note: Around the world a variety of other frequencies are used for both analog and digital hand-held transceivers and mobile radios, and other names are given to the systems (see Table 1 in Stuchly [83] for details). The most common frequencies for "cellular" systems are 800-900 MHz (analog and digital) and 1800-2000 MHz (digital); but hand-held transceivers exist that use frequencies from as low as 45 MHz to as high as 2500 MHz. Power output from hand-held units seldom exceeds 2 W, but power output from vehicle-mounted units such as those used by law enforcement personnel can be as high as 100 W.
Canada: Analog and digital phones operate at 824-849 MHz. A 2000 MHz digital system (similar or identical to PCS service in the US) is coming soon.
Australia: The analog AMPS phones operate at 825-890 MHz and the digital GSM phones operate at 890-960 MHz.
Europe: Analog systems at about 900 MHz; digital (GSM) systems at about both 900 and 1800 MHz.
3. The specific frequencies used by cellular and PCS phones can be called either microwaves (MW), radiofrequencies (RF), or radiowaves. For the discussion of health effects the distinction between radiowaves and microwaves is semantic, and the term radiowaves (or radiofrequency or RF) is used in this document for all frequencies between 3 kHz and 300 GHz.
4. For a detailed discussion see:
- JE Moulder and KR Foster: Biological effects of power-frequency fields as they relate to carcinogenesis. Proc Soc Exper Biol Med 209:309-324, 1995;
- JE Moulder: Power-frequency fields and cancer. Crit Rev Biomed Engineering 26:1-116, 1998.
5. IEEE Standards Coordinating Committee 28 on Non-Ionizing Radiation Hazards: Standard for safety levels with respect to human exposure to radio frequency electromagnetic fields, 3 kHz to 300 GHz (ANSI/IEEE C95.1-1991), The Institute of Electrical and Electronics Engineers, New York, 1992.
6. International Commission on Non-Ionizing Radiation Protection: Guidelines for limiting exposure to time-varying electric, magnetic and electromagnetic fields. Health Physics 74:494-522, 1998.
7. National Council on Radiation Protection and Measurements: Biological effects and exposure criteria for radiofrequency electromagnetic fields. NCRP Report No. 86, 1986.
8. The biological effects of radiowaves depend on the rate at which power is absorbed. This rate of energy absorption is called the Specific Absorption Rate (SAR) and is measured in watts/kilogram (W/kg). SARs are difficult to measure on a routine basis, so what is usually measured is the plane wave power density. Average whole body SARs can then be calculated from the power density exposure (see Stuchly [83] for details).
Note that some documents express power density as W/cm-sq, where 1000 W/cm-sq equals 1 mW/cm-sq.
9. The power density standards are stricter for cellular frequencies than for PCS frequencies because humans absorb radiowaves more at 860 MHz than at 1800 MHz, and it is the amount of power absorbed that really matters [8].
10. Specifically, the ICNIRP standard is 0.40 mW/cm-sq for cellular phone frequencies and 0.90 mW/cm-sq for PCS phone frequencies, while the NCRP guideline is 0.57 mW/cm-sq for cellular phone frequencies and 1.00 mW/cm-sq for PCS phone frequencies.
11. Guidelines for Evaluating the Environmental Effects of Radiofrequency Radiation (FCC 96-326), Federal Communications Commission, Washington, D.C., 1996. Available from the FCC web page.
12. Specifically, the new FCC standard is 0.57 mW/cm-sq for cellular phone frequencies and 1.0 mW/cm-sq for PCS phone frequencies.
International note: A number of countries have their own regulations. While these regulations generally follow the same patterns and rationales used by ANSI/IEEE [5] and ICNIRP [6], they do differ.![]() Australian standard:
Australian standard:
The Australian situation is rather complex. Until 1998, RF exposure in Australia was regulated by "AS2772.1-1990 Radiofrequency radiation, Part 1: Maximum exposure levels-100 kHz to 300 GHz including Amendment No. 1/1994" from the Standards Association of Australia. In that standard the allowable general public exposure limit for the frequencies used by mobile phone services was 0.2 mW/cm-sq; this was a factor of 2 - 6 lower than the FCC, ANSI/IEEE, ICNIRP and NCRP standards.
This standard was revised in 1998 on an interim basis, and the allowable general public exposure limits in the new "interim" standard [AS/NZS2772.1(Int):1998] appeared to similar to the ICNIRP standard [6] except at higher frequencies where the lower limits of the 1990 Standard were retained. This interim standard was effective until 5-March-99, when it was to have been "confirmed, withdrawn or revised". The committee responsible for the standard was unable to achieve the required level of consensus to confirm or revise the interim standard and it was subsequently withdrawn.
When the AS/NZS2772.1(Int):1998 lapsed, the Australian Communications Authority (ACA) stepped in and adopted its own radiocommunications RF standard. The ACA standard appears to be largely identical to AS/NZS2772.1(Int):1998, except that it applies only to RF used for communications.
New Zealand standard:
In 1998 the Australian and New Zealand standards were merged as an "interim" standard [AS/NZS2772.1(Int):1998]. The same confusion that applied to the Australian standard occurred in New Zealand. However, unlike Australia, New Zealand has adopted a final standard, "NZS 2772.1:1999 Radiofrequency fields - Part 1: Maximum exposure levels - 3 kHz to 300 GHz", that aligns fully with the ICNIRP Guidelines [6] and does not contain the reduced exposure levels at higher frequencies that were part of the earlier standards.
Canadian standard: Health Canada: Limits of exposure to radiofrequency fields at frequencies from 10 kHz - 300 GHz Safety Code 6, Canada Communication Group, Ottawa, Canada, (1993). At the frequencies of relevance to base stations the Canadian standard appears to be identical to the FCC standard.
UK standard: The UK standard [14] is 0.57 mW/cm-sq at 900 MHz and 1.00 mW/cm-sq at 1800 MHz.
13. Where there are multiple transmitting antennas at different frequencies, the method for assuring adherence to the ANSI [5] or FCC [11] standards is complex. However, there is also an easy way to check adherence under these conditions: add the power densities of all the antennas and apply the strictest power density standard. Anything which passes this easy check will pass the more stringent and complex test. Something that fails this easy check must be analyzed by the more stringent and complex method described in the ANSI standard.
14. National Radiation Protection Board: Restrictions on human exposure to static and time varying electromagnetic fields and radiation. Doc NRPB 4:1-69, 1993.
15. The 1992 ANSI standard [5], for example, is based on the review of 321 papers from the peer-reviewed literature; and the NCRP guidelines [7] are based on a review of nearly 1000 reports.
16. Specifically, no potentially-hazardous effects have been reproducibly shown below a SAR of 4 W/kg.
- At cellular and PCS phone frequencies it would require a power density of 20-100 mW/cm-sq to achieve a SAR as high as 4 W/kg.
- Under worst-case assumptions (multiple low-gain, high-ERP antennas), the SAR of a human in publicly-accessible locations near a FCC-compliant base station would be less than 0.01 W/kg.
- Under realistic conditions the SAR to a human near such a base station would be less than 0.0005 W/kg.
17. ANSI, ICNIRP and NCRP all agree that whole body exposure of the general public should be kept below a whole body SAR of 0.08 W/kg. Where the standards disagree is about the specific relationship of SAR to power-density, a relationship that is determined from a combination of dosimetry and biophysical modeling.
International note: As a result of differences between approaches and frequencies used, world-wide standards for the continuous exposure of the public to RF from base station antennas ranges from 0.20 to 1.20 mW/cm-sq.
18. For the "panel" antennas used by most PCS base stations, the area of concern is only at the front of the antennas. For the "whip" style antennas used in many cellular base station antennas, the area of concern would be in all directions. This differences becomes clearer after an examination of the RF patterns from each type of antenna (see Q14C).
These general statements about minimum safe distances assume that total ERPs per sector for base station antennas will not exceed 2000 W. In the U.S., this is generally the case; and under the U.S. FCC guidelines, sites with total ERPs above 2000 W will require specific site evaluations [see note 19].
International note: More powerful antennas may be used elsewhere, in which case the minimum safe distances would be larger. Minimum safe distances will also be larger when there are multiple antennas broadcasting in the same sector.
19. Specifically, the FCC will require evaluations for:
International note: Strictly speaking, these criteria only apply in the U.S. Nevertheless, they are useful criteria for determining what types of antenna sites are most likely to violate RF standards. For example, sites that are exempted from measurement requirement under the FCC rules should also easily meet the stricter Australian standard.
20. One distinction that is often made in discussions of the biological effects of radiowaves is between "nonthermal" and "thermal" effects. This refers to the mechanism for the effect: non-thermal effects are a result of a direct interaction between the radiowaves and the organism, and thermal effects are a result of heating. There are some reported biological effects of radiowaves whose mechanisms are unknown, and it is difficult (and not very useful) to try to draw a distinction between "thermal" and "nonthermal" mechanisms for such effects.
21. These effects have included changes in the electrical activity of the brain, changes in enzyme activity, and changes in calcium ion transport across membranes [for details see 1, 5, 6, 7 and 14].
22. Santani et al: Electric fields from 900 MHz digital cellular telephones. Bioelectromagnetics Society, Tampa, June 1998.
23. The increased human absorption at 900 MHz (U.S. cell phone frequency) versus 2000 MHz (U.S. PCS phone frequency) applies to whole body exposure at a distance from the antenna (the case for public exposure near a base station antenna site). This difference may not apply to partial body exposures in very close proximity to an antenna.
![]() 24. WR Adey, CV Byus et al: Spontaneous and nitrosourea-induced primary tumors of the central nervous system in Fischer 344 rats chronically exposed to 836 MHz modulated microwaves. Radiat Res 152:293-302, 1999.
24. WR Adey, CV Byus et al: Spontaneous and nitrosourea-induced primary tumors of the central nervous system in Fischer 344 rats chronically exposed to 836 MHz modulated microwaves. Radiat Res 152:293-302, 1999.
25a. KH Mild et al: Use of mobile phones and subjective disorders. A Swedish-Norwegian epidemiological study. Background and development of questionnaire. Bioelectromagnetic Society, Tampa, June 1998.
25b: M Sandstrm et al: Subjective symptoms among mobile phone users in Sweden and Norway. A Swedish-Norwegian epidemiological study. Bioelectromagnetic Society, Tampa, June 1998.
26a. BJ Youbicier-Simo, JC Lebecq and M Bastide: Mortality of chick embryos exposed to EMFs from mobile phones. Bioelectromagnetic Society, Tampa, June 1998.
26b. BJ Youbicier-Simo, JC Lebecq and M Bastide: Damage of chicken embryos by EMFs from mobile phones: Protection by a compensation antenna. Bioelectromagnetic Society, Tampa, June 1998.
27. See 63b.
28. B Hocking et al: Cancer incidence and mortality and proximity to TV towers. Med J Austral 165:601-605, 1996.
29A. JR Goldsmith: Epidemiologic evidence of radiofrequency (microwave) effects on health in military, broadcasting, and occupational studies. Int J Occup Environ Health 1:47-57, 1995.
JR Goldsmith: Epidemiologic evidence relevant to radar (microwave) effects. Environ Health Perspec 105:1579-1587, 1997.
30. A discussion of the problems with interpreting ecological epidemiology studies is beyond the scope of document. For discussion of this issue see:
S Piantadosi et al: The ecological fallacy. Am J Epidem. 127(5):893-904, 1988.
S Schwartz: The fallacy of the ecological fallacy: the potential misuse of a concept and the consequences. Am J Public Health. 84(5):819-24, 1994.
31a. H Lai and NP Singh: Acute low-intensity microwave exposure increases DNA single-strand breaks in rat brain cells. Bioelectromag 16:207-210, 1995
31b. H Lai and NP Singh: Single- and double-strand DNA breaks in rat brain cells after acute exposure to radiofrequency electromagnetic radiation. Int J Rad Biol 69:513-521, 1996.
32. A Maes et al: 954 MHz microwaves enhance the mutagenic properties of mitomycin C. Environ Molec Mutagen 28:26-30, 1996.
33. JK Grayson: Radiation exposure, socioeconomic status, and brain tumor risk in US Air Force: A nested case-control study. Amer J Epidem 143:480-486, 1996.
34. H Dolk et al: Cancer incidence near radio and television transmitters in Great Britain I. Sutton Coldfield Transmitter. Amer J Epidem 145:1-9, 1997.
35. H Dolk et al: Cancer incidence near radio and television transmitters in Great Britain. II. All high power transmitters. Amer J Epidem 145:10-17, 1997.
36. MR Scarfi et al: Genotoxic effects of mitomycin-C and microwave radiation on bovine lymphocytes. Electro Magnetobio 15:99-107, 1996.
37. MH Repacholi et al: Lymphomas in E-Pim1 Transgenic Mice Exposed to Pulsed 900 MHz Electromagnetic Fields. Rad Res 147:631-640, 1997.
38. Quotes from the abstract of Repacholi et al [37] :
"...One hundred mice were sham-exposed and 101 were exposed for two 30-min periods per day for up to 18 months to plane wave fields of 900 MHz with a pulse repetition frequency of 217 Hz and a pulse width of 0.6 ms. Incident power densities were 0.26-1.3 mW/cm-sq and [average SAR was] 0.13-1.4 W/kg. Lymphoma risk was found to be significantly higher in the exposed mice than in the controls (OR=2.4, p=0.006, 95% CI=1.3-4.5)... Thus long-term intermittent exposure to RF fields can enhance the probability that mice carrying a lymphomagenic oncogene will develop lymphomas".
39. Quotes from the discussion in Repacholi et al [37]
"[the literature] does not seem to offer a mechanism by which RF field exposure... could increase the incidence of lymphoid malignancy"
"While the increase in the incidence of lymphoma found here was highly significant statistically, and the exposure conditions were designed to mimic the fields generated by a digital mobile telephone, the implications of the study for risk of carcinogenesis in humans are unclear. It is difficult to extrapolate directly from mice to humans due to differences in their absorption of energy from RF fields."
"We would not interpret these studies as indicating that RF-field exposure would be specifically lymphomagenic in normal animals."
"That is not to imply that any humans at all are necessarily at increased risk of cancer as a consequence of exposure to RF fields. No single experiment on animals can allow such a conclusion."
40. Further technical notes concerning Repacholi et al [37]:
- Mice used in these studies are transgenic animals that are born with an activated oncogene that predisposes them to develop lymphoma. By the age of 10 months 5-10% of these mice develop lymphomas, and by 18 months about 15% develop lymphomas. The incidence of lymphoma in normal mice is very much lower.
- The data analysis was blinded. The exposures themselves were not completely blinded; during the course of the experiments the investigators knew which mice were being exposed and which were not, but the people caring for the animals did not.
- The RF field was not uniform in the exposure room, and the animals were allowed to move freely in their cages during the exposure. As a result, the actual exposure levels of the animals are not known. All that is known is that the SAR range was 0.007 to 4.3 W/kg and that the average SAR for the mice was 0.14 to 1.4 W/kg.
- The ANSI/IEEE standard for exposure of the general public to RF is based on keeping exposures below 0.08 W/kg. The SAR level in publicly-accessible locations near cellular phone or PCS base stations is in the 0.0005-0.005 W/kg range [16]. Thus the exposure levels used in this mouse study are well above those to which people are actually exposed.
- Because the animals used in the study are genetically predisposed to lymphoma it is difficult to decide whether this should be viewed as a test for genotoxic activity or a test for epigenetic activity (see thepower lines-cancer FAQ for a discussion of the distinction).
41a. Vijayalaxmi et al: Frequency of micronuclei in the peripheral blood and bone marrow of cancer-prone mice chronically exposed to 2450 MHz radiofrequency radiation. Rad Res 147:495-500, 1997.
41b. Vijayalaxmi et al: Proliferation and cytogenetic studies in human blood lymphocytes exposed in vitro to 2450 MHz radiofrequency radiation. Int J Rad Biol 72:751-757, 1997.
42. CD Cain et al: Focus formation of C3H/10T1/2 cells and exposure to a 836.55 MHz modulated radiofrequency field. Bioelectromag 18:237-243, 1997.
43. CK Chou et al: Long-term, low-level microwave irradiation of rats. Bioelectromag 13:469-496, 1992.
44. MR Frei et al: Chronic exposure of cancer-prone mice to low-level 2450 MHz radiofrequency radiation. Bioelectromag. 19, 20-31, 1998.
45. JC Toler et al: Long-term low-level exposure of mice prone to mammary tumors to 435 MHz radiofrequency radiation. Rad Res 148:227-234, 1997.
46. DL Hayes et al: Interference with cardiac pacemakers by cellular telephones. New Eng J Med 336:1473-1479, 1997.
47. MR Frei et al: Chronic low-level (1.0 W/Kg) exposure of mammary cancer-prone mice to 2450 MHz microwaves. Rad Res 150:568-576, 1998.
48. AH Frey: Commentary: Headaches from cellular telephones: Are they real and what are the implications? Environ Health Perspec 106:101-103, 1998.
49a. RS Malyapa et al: Measurement of DNA damage following exposure to 2450 MHz electromagnetic radiation. Rad Res 148:608-617, 1997.
49b. RS Malyapa et al: Measurement of DNA damage following exposure to electromagnetic radiation in the cellular communications frequency band (835.62 and 847.74 MHz). Rad Res 148:618-627, 1997.
49c. RS Malyapa et al: DNA damage in rat brain cells after in vivo exposure to 2450 MHz electromagnetic radiation and various methods of euthanasia. Rad Res 149:637-645, 1998.
50. WR Adey et al: Brain tumor incidence in rats chronically exposed to frequency-modulated (FM) cellular phone fields. 2nd World Congress, Bologna, 1997.
51. T Shirai et al: Lack of promoting effects of the electromagnetic near-field used for cellular phones (929 MHz) on rat liver carcinogenesis in medium-term bioassay. 2nd World Congress, Bologna, 1997.
52. G d'Ambrosio et al: Preliminary results on human lymphocytes exposed in vitro to cellular telephone microwave frequency. 2nd World Congress, Bologna, 1997.
53. KR Foster, LS Erdreich and JE Moulder: Weak electromagnetic fields and cancer In the context of risk assessment. Proc IEEE 85:731-746, 1997.
54. Measurements show that signal strength in a building is anywhere from 5% to 40% of the level measured in the street outside. In general, signal attenuation is greater at ground level than higher up in the building, and attenuation is less at higher (PCS) frequencies than at lower (cell phone) frequencies (JD Parsons, The Mobile Phone Propagation Channel, Wiley and Sons, NY, 1992).
55. A worst-case calculation (2000 W ERP low-gain antenna mounted directly on a low-attenuation roof) predicts a power density of less than 0.10 mW/cm-sq on the floor below. A calculation for a more typical roof-top mount (1000 W ERP high-gain antenna, mounted 2 meters above a typical roof) predicts a power density of less than 0.001 mW/cm-sq on the floor below.
Actual measurements in the top floor apartments of a building with high-gain (panel) base stations antennas mounted to the outside of the parapet just above the apartments found a maximum power density of 0.0004 mW/cm-sq [101]. Measurements in a corridor in the floor directly below a roof-top base station (antennas 3 meters above the main roof) found a maximum power density of 0.008 mW/cm-sq. Both maximums assume that the base stations are operating at their maximum capacity of 2000 W ERP [101].
56. RY Wu et al: Effects of 2.45 GHz microwave radiation and phorbol ester 12-O-tetradecanoylphorbol-13-acetate on dimethylhydrazine -induced colon cancer in mice. Bioelectromag 15:531-538, 1994.
57. ED Mantiply et al: Summary of measured radiofrequency electric and magnetic fields (10 kHz to 30 GHz) in the general and work environment. Bioelectromag 18:563-577, 1997.
58. R Coghill: Something in the Air: A Biologists Review of Adverse and Beneficial Effects on Mankind, Nature and the Environment, From the Use of Radio, TV, Telecommunications, Mobile Phones, Microwaves and Electricity. Source and publisher obscure, 1997?
59. Quotes are from EMF Health and Safety Digest, Sept 1997, pp 12-13.
60. N Cherry: Potential adverse health effects of cell sites". Source and publisher obscure, 1996?.
61. Quotes are from an internet "interview" in NZine (www.nzine.co.nz) in July of 1997.
62. DR McKenzie et al: Childhood incidence of acute lymphoblastic leukemia and exposure to broadcast radiation in Sydney -- a second look. Aust New Zealand J Public Health 22:360-367, 1998.
63a. K Imaida et al: Lack of promoting effects of the electromagnetic near-field used for cellular phones (929.2 MHz) on rat liver carcinogenesis in a medium-term liver bioassay. Carcinogenesis 19:311-314, 1998.
63b. K Imaida et al: The 1.5 GHz electromagnetic near-field used for cellular phones does not promote rat liver carcinogenesis in a medium-term liver bioassay. Jap J Cancer Res 89:995-1002, 1998.
64. JF Spalding et al: Effects of 800-MHz electromagnetic radiation on body weight, activity, hematopoiesis and life span in mice. Health Phys 20:421-424, 1971.
65. S Szmigielski et al: Accelerated development of spontaneous and benzopyrene-induced skin cancer in mice exposed to 2450 MHz microwave radiation. Bioelectromag 3:179-191, 1982.
66. CG Liddle et al: Alteration of life span of mice chronically exposed to 2.45 GHz CW microwaves. Bioelectromag 15:177-181, 1994.
67. CD Robinette et al: Effects upon health of occupational exposure to microwave radiation. Amer J Epidem 112:39-53, 1980.
68. DA Hill: Longitudinal study of a cohort with past exposure to radar: the MIT Radiation Laboratory follow-up study [dissertation], University of Michigan Dissertation Service, Ann Arbor, Michigan, 1988.
69. S Milham: Increased mortality in amateur radio operators due to lymphatic and hematopoietic malignancies. Amer J Epidem 127:50-54, 1988.
70. AM Lilienfeld et al: Foreign Service Health Status Study - Evaluation of Health Status of Foreign Service and Other Employees from Selected Eastern European Posts. Final Report, Contract No. 6025-619073, United States Department of Health, Washington, D.C., 1978.
71. S Lagorio et al: Mortality of plastic-ware workers exposed to radiofrequencies. Bioelectromag 18:418-421, 1997.
72. JM Muhm: Mortality investigation of workers in an electromagnetic pulse test program. J Occup Med 34:287-292, 1992.
73. T Tynes et al: Incidence of cancer in Norwegian workers potentially exposed to electromagnetic fields. Amer J Epidem 136:81-88, 1992.
74. MH Repacholi: Radiofrequency field exposure and cancer: What do the laboratory studies suggest? Environ Health Perspec 105:1565-1568, 1997.
75. A Antonopoulos et al: Effects of high-frequency electromagnetic fields on human lymphocytes in vitro. Mut Res 395:209-214, 1997.
76. S Kwee and P Rasmark: Changes in cell proliferation due to environmental non-ionizing radiation 2. Microwave radiation. Bioelectrochem Bioenerg 44:251-255, 1998.
77. RC Petersen et al: Radio-frequency electromagnetic fields associated with cellular-radio cell-site antennas. Bioelectromag 13:527-542, 1992.
78. JL Phillips et al: DNA damage in Molt-4 T-lymphoblastoid cells exposed to cellular telephone radiofrequency fields in vitro. Bioelectrochem Bioenerg 45:103-110, 1998.
79. S Szmigielski: Cancer morbidity in subjects occupationally exposed to high-frequency (radiofrequency and microwave) electromagnetic radiation. Sci Total Environ 180:9-17, 1996.
80. L Verschaeve and A Maes: Genetic, carcinogenic and teratogenic effects of radiofrequency fields. Mut Res 410:141-165, 1998.
81. D Brusick et al: Genotoxicity of radiofrequency radiation. Environ Molec Mutagen 32:1-16, 1998.
82. S Braune et al: Resting blood pressure increase during exposure to a radiofrequency electromagnetic field. Lancet 351(9119):1857-1858, 1998.
83. MA Stuchly: Biological concerns in wireless communications. Crit Rev Biomed Eng 26:117-151, 1998.
84. C Eulitz et al: Mobile phones modulate response patterns of human brain activity. NeuroReport 9:3229-3232, 1998.
85. OM Garson, TL McRobert et al: A chromosomal study of workers with long-term exposure to radio-frequency radiation. Med J Austral 155:289-292, 1991.
86. IN Magras and TD Xenos: RF radiation-induced changes in the prenatal development of mice. Bioelectromag 18:455-461, 1997.
87. PC Goswami, LD Albee et al: Proto-oncogene mRNA levels and activities of multiple transcription factors in C3H 10T1/2 murine embryonic fibroblasts exposed to 835.62 and 847.74 MHz cellular phone communication frequency radiation. Radiat Res 151:300-309, 1999.
88. S Ray and J Behari: Physiology changes in rats after exposure to low levels of microwaves. Radiat Res 123:199-202, 1990.
89. SK Dutta, B Ghosh et al: Radiofrequency radiation-induced calcium ion efflux enhancement from human and other neuroblastoma cells in culture. Bioelectromag 10:197-202, 1989.
90. J Juutilainen and R de Seze: Biological effects of amplitude-modulated radiofrequency radiation. Scand J Work Environ Health 24:245-254, 1998.
91. JL Chagnaud and B Veyret: In vivo exposure of rats to GSM-modulated microwaves: flow cytometry analysis of lymphocyte subpopulations and of mitogen stimulation. Int J Radiat Biol 75:111-113, 1999.
92. H Lai, A Horita et al: Microwave irradiation affects radial-arm maze performance in the rat. Bioelectromag 15:95-104, 1994.
93. H Lai: Research on the neurological effects of nonionizing radiation at the University of Washington. Bioelectromag 13:513-526, 1992.
94. JM Elwood: A critical review of epidemiologic studies of radiofrequency exposure and human cancers. Environ Health Perspect 107(Suppl. 1):155-168, 1999.
95. JE Moulder, LS Erdreich et al: Cell phones and cancer: What is the evidence for a connection? Radiat. Res., 151:513-531,1999.
On line version available.
96. JA D'Andrea: Behavioral evaluation of microwave irradiation. Bioelectromag 20:64-74, 1999.
97. AW Preece, G Iwi et al: Effect of a 915-MHz simulated mobile phone signal on cognitive function in man. Int J Radiat Biol 75:447-456, 1999.
98. RD Saunders, CI Kowalczuk et al: Studies on the induction of dominant lethals and translocations in male mice after chronic exposure to microwave radiation. Int J Radiat Biol 53:983-992, 1988.
99. Royal Society of Canada: A review of the potential risks of radiofrequency fields from wireless telecommunication devices. Royal Society of Canada, Ottawa, Ont, (http://www.rsc.ca)
100. L Hardell, A N'sman et al: Use of cellular telephones and the risk of brain tumors: a case-control study. Int. J. Oncol. 15:113-116, 1999.
101. RC Petersen, AK Fahy-Elwood et al: Wireless telecommunications: Technology and RF safety issues, In: "Non-Ionizing Radiation: An Overview of the Physics and Biology", KA Hardy, ML Meltz et al (editors), Medical Physics Publishing, Madison, WI, pp. 197-226,1997.
Ways to save money AND help the environment:
Save water AND money with this showerhead adapter, it lets the water flow until the water is hot, then shuts off water flow until you restart it, ShowerStart TSV Hot Water Standby Adapter
it lets the water flow until the water is hot, then shuts off water flow until you restart it, ShowerStart TSV Hot Water Standby Adapter

Protect your health with these:
Mattress Dust mite-Bedbug protector, 100% Waterproof, Hypoallergenic, Zippered
Handheld Allergen Vacuum Cleaner with UV Sanitizing for Allergies and Pet, Kills Mite, Virus, Molds, True HEPA with Powerful Suction removes Hair, Dander, Pollen, Dust ,
,
Immune Support Supplement with Quercetin, Vitamin C, Zinc, Vitamin D3
GermGuardian Air Purifier with UV-C Light and HEPA 13 Filter, R emoves 99.97% of Pollutants
emoves 99.97% of Pollutants
HEPA Air Purifier, HEPA Air Cleaner with Washable Pre-Filter, AQI Display, ECO Mode, Sleep Mode, Pet Mode for Pets, Dust, Pollen, Removes 99.97% of Particles, Smoke, Mold, Pet Dander, Dust, Odors
Interesting Reads:
THE PREPPER'S CANNING & PRESERVING BIBLE: [13 in 1] Your Path to Food Self-Sufficiency. Canning, Dehydrating, Fermenting, Pickling & More, Plus The Food Preservation Calendar for a Sustainable Pantry
The Backyard Homestead: Produce all the food you need on just a quarter acre! P aperback
aperback
The Citizens' Guide to Geologic Hazards: A Guide to Understanding Geologic Hazards Including Asbestos, Radon, Swelling Soils, Earthquakes, Volcanoes
The Uninhabitable Earth: Life After Warming
Book: The Sixth Extinction:
An Unnatural History Paperback
 .
.